Iron deficiency anaemia occurs when the iron stores are so empty that there is not enough iron to make proper new red blood cells. The new red blood cells are thus fewer, smaller and paler and cannot carry oxygen effectively. Your body will always prioritize the available iron to first be used in the red blood cells, but iron has many other functions in the body (see previous post). So by the time that there is iron deficiency anaemia, the brain especially has already suffered from the lack of iron. (See previous blog post for more information about Iron Deficiency in general.)
This is a sneaky disease because there are almost no symptoms initially. It is thus important that your doctor asks about the risk factors for developing iron deficiency during well-child-visits.
Babies and toddlers between the age of 6months to 3years have an especially high risk to develop iron deficiency anemia. The American Association of Pediatrics recommend that all children should be screened between 9-12 months of age because of the serious effects it has on long term neurodevelopment. Several studies show that the delays in development improves with treatment, but does not normalise completely.
The most common cause of iron deficiency is insufficient intake (see previous post for tips on prevention). Other causes could be blood loss from the gut, specific syndromes where iron is not absorbed from the gut or chronic inflammatory diseases.
Symptoms of Iron deficiency anaemia:
Mild:
- No specific symptoms
- Iron deficiency could lead to behavioural changes in your child that is sometimes difficult to pin-point eg. children become more wary, hesitant, solemn, unhappy, keep closer to their mothers.
- Restless leg syndrome, breath holding spells, sleep disturbances, short attention span, learning difficulties have also been seen to improve when iron deficiency was treated.
- Pica : an intense craving for weird non-food items such as clay, dirt, chalk, soap, paper, raw rice or ice (pagophagia). No one knows how this works, but it responds very well to iron supplementation.
- Poor growth
Severe:
- Pallor (seen especially around the eyes, in the mouth, the nails and on the palms/soles)
- Severe tiredness and loss of interest in otherwise fun activities
- Irritability
- Poor appetite, sores in the corners of the mouth, painful tongue
- Fast heartbeat, heart failure, fast breathing.
Other complications associated with iron deficiency anaemia:
- Febrile seizures (although no relational cause could be found, several studies have found that children with febrile seizures are more prone to be iron deficient)
- Iron deficiency causes paralysis of some parts of the immune system
If your doctor suspects iron deficiency anaemia, blood tests will be the next step to confirm. A hemoglobin or full-blood count and ferritin count will be enough. Treatment with Iron supplements can then be started and the effect on the red blood cells will be evaluated after one month of treatment. If there are no response further investigations should be done for other causes of the anemia.
Treatment of iron deficiency anaemia:
- Ferrous sulphate 3-6mg dly (can be given once a day or in divided dosages.)
The best absorption of iron happens when you give it with orange juice (or other juice high in Vitamin C as this improves absorption) in between meals. Foods that can block absorption of iron are dairy, eggs, tea or coffee, whole-grain breads and cereals / bran.
Iron supplements are notorious for having many side effects. However if you start at a low dose and slowly increase it, and give the iron with meals, most children tolerate it quite well. Remember to give the drops at the back of your child’s mouth or give it mixed in juice with a straw. Some iron supplements may stain the teeth, but this can be removed by brushing with baking soda (talk to your dentist first). There are many different iron formulations of which some are better absorbed/better tolerated, but this also comes with a significant price increase. In the end the most important thing is that your child drinks the supplement. (Studies show no difference in the end-result for different formulations).
VERY IMPORTANT: Treatment for iron deficiency anaemia should be given for at least 3months, even if the blood count normalises before that. Remember that the body will use any available iron for the red blood cells first, and then the stores still need to be filled to prevent future problems.
- Dietary advice
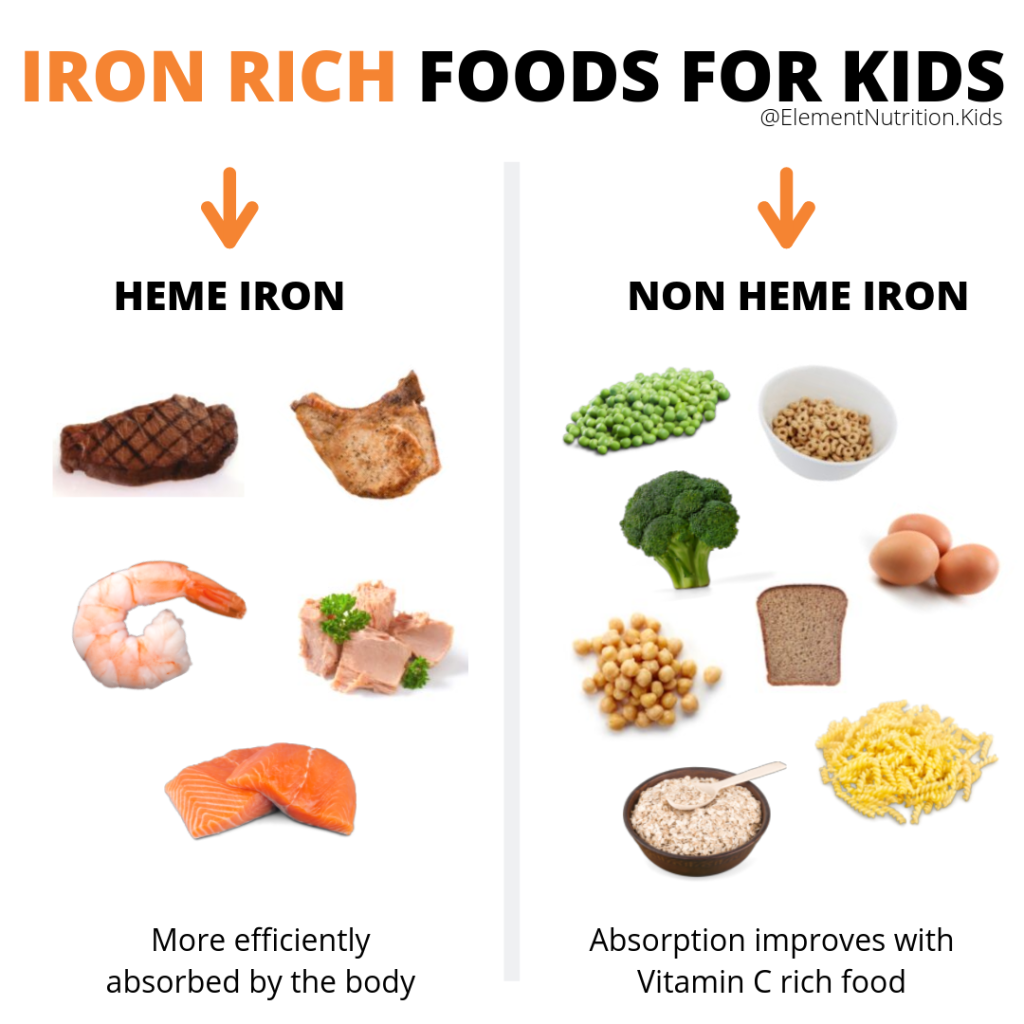
It is important that your child’s diet is also adapted to include more iron rich foods. It is adviced that they should eat at least 2-3 iron rich meals per day. Remember that the iron in animal products is absorbed better and thus you need to eat bigger quantities of plant-based iron to absorb the same amount.
Some foods that are high in iron include:
- Meat – red and white. Liver is especially high in iron.
- Other animal sources: Eggs (especially the yolk), fish
- Dried fruits: raisins, apricots
- Green leafy vegetables
- Dried beans and lentils
- Oats, other grains
- Soybeans
I hope you now feel more confident in the whys and hows of iron deficiency. There are still so many ongoing studies and new developments with regards to the influence and treatment of different neurodevelopmental diseases such as autism and ADHD that I am sure this is a topic that we will still hear a lot about!
- Ozdemir N; “Iron deficiency anemia from diagnosis to treatment in children”; Turk Pediatri Ars; 2015 Mar; 50(1): 11-19
- www.uptodate.com
- https://www.mayoclinic.org/drugs-supplements/iron-supplement-oral-route-parenteral-route/description/drg-20070148
