When Eran was 8 months old we woke one night to a cot full of vomit. Things deteriorated from there. Two days of diarrhoea (with stools leaking through everything) and vomiting with a mild fever followed. I am grateful that it was a very mild episode and he was never dehydrated, but I still had a lot of worry and washing! I have spent many nights admitting children to ICU with severe dehydration and I know how fragile they are, but there is a lot you can do at home to prevent a crisis. Let us look at the how and why of diarrhoea.

According to the WHO the definition of diarrhoea is 3 or more loose or watery stools per day, or any change from the child’s usual stool patterns. (I explained the big variety of normal stool patterns in my blogpost about constipation.) Diarrhoea is still one of the top 5 causes of childhood death in children under 5 years in the developing world and should always be taken seriously.
“Looking after a very sick child was the Olympics of parenting.”
Chris Cleave
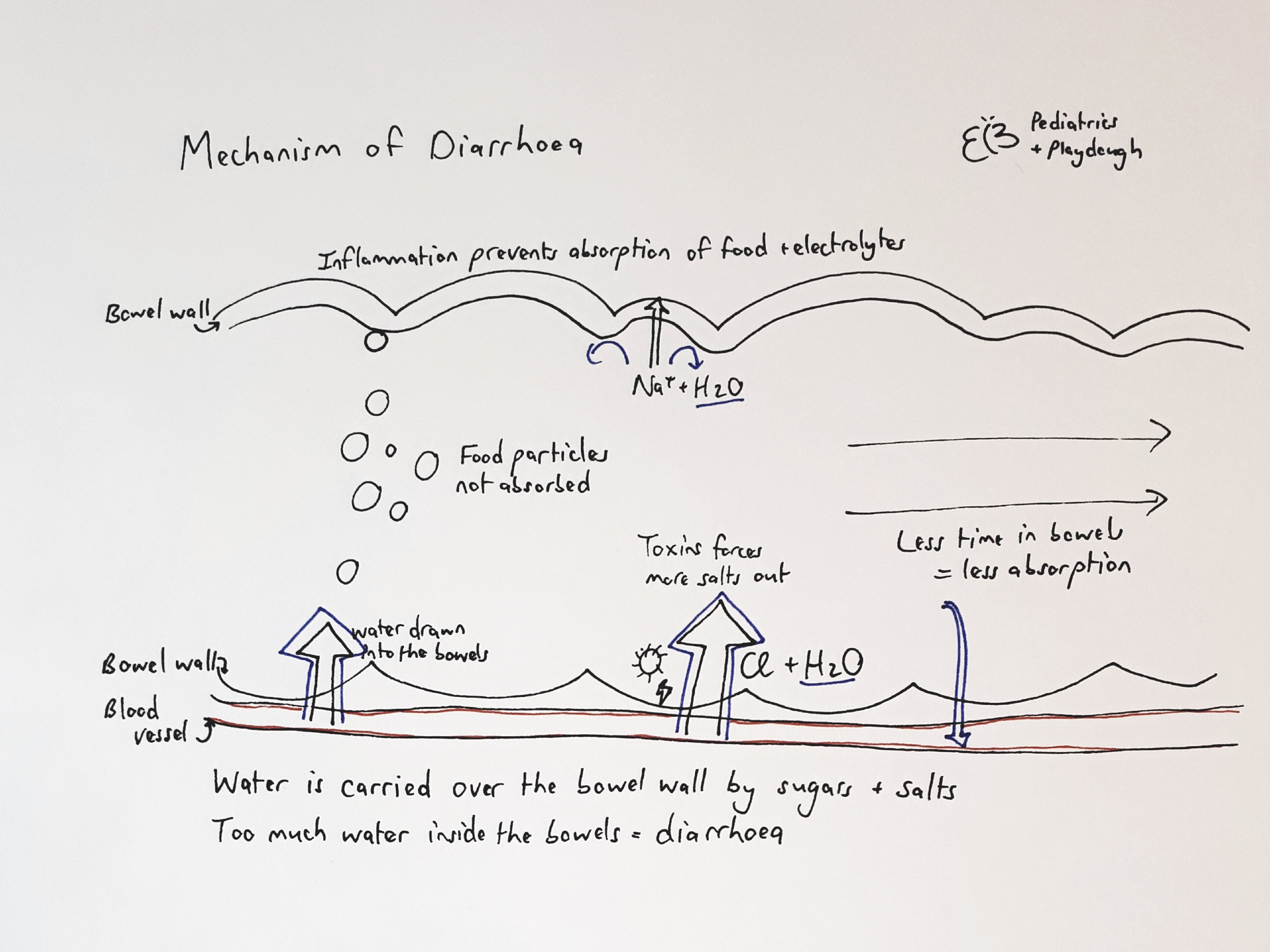
Why does children get diarrhoea? The main function of both the small and large intestines are to absorb/ expell water to maintain a normal fluid balance in the body. Water is carried over the bowel wall by electrolytes (salts such as Sodium, Potassium, Chloride) and by sugars (Glucose). Water is also drawn into the bowel cavity by particles (such as carbohydrates or laxatives) that is not absorbed into the body.
Diarrhoea starts when there is an excess of water in the bowel cavity. Viruses or bacteria (such as the rotavirus or cholera bacteria) forms toxins which forces too many electrolytes out of the body, followed by water. Infection causes inflammation (swelling) of the bowel wall, causing less absorption of sugars and electrolytes, and thus more water in the bowel cavity. Infection or medications can also irritate the bowels, causing more frequent contractions and thus a shorter transit time of food and fluids, thus more water stays in the bowel.1
The microbiome of good bacteria in the colon (large intestine) also plays a big role in water absorption. It helps with fermentation of the carbohydrates that were not absorbed in the small intestine and changes it into smaller pieces that can be used by the body. It is then absorbed together with water. If this microbiome is disturbed, it can lead to diarrhoea.
Still with me? It can be confusing with all the in and out-movements of the water, but basically it all causes outward movement of smelly fluids from the mouth or bum of your baby! When you understand the mechanisms, you will also understand why certain treatments work. I hope this sketch helps:
Diarrhoea can be divided into acute (continues for less than 5-7 days), intermittent (7-28 days) and chronic (>4weeks).
Acute diarrhoea in children is mostly caused by viral infections (up to 60-70% of moderate to severe cases of diarrhoea in children under 2years)2. The children usually have some vomiting, watery stools and a mild fever (38-39°C). There are many different viruses involved, but thankfully the more severe rotavirus diarrhoea has decreased after the introduction of immunisations, keeping many small babies out of the hospital. Most children with a viral diarrhoea only need supportive treatment and the disease usually clears up spontaneously within a few days.
Bacterial infections are the cause of diarrhoea in 30% of cases in children between 2-5years. These kids are almost always more toxic (high fevers above 40°C, looks ill, severe stomach pain, blood or mucous in the stools). The diagnosis can be made with stool or blood cultures.
Another common cause of acute diarrhoea is antibiotic-associated diarrhoea. It usually starts during or shortly after a course of antibiotics such as Amoxicillin or Amoxicillin with clavulanic acid. The diarrhoea is due to a disturbance in the microbiome in the colon as described above or could be due to a secondary infection due to overgrowth of a “bad bacteria” because the antibiotic wiped out all the “good bacteria” from the colon.
When your baby starts to spew bodily fluids all over the place, I am sure you don’t really care so much about the cause, so let me tell you the things to look out for and when to start worrying.
If your child has any of the following symptoms when they have diarrhoea, please see a doctor as it could indicate a cause that need specific treatment:
- Blood in the stools (could indicate a bacterial or serious gut disease that needs urgent treatment)
- Mucous in the stools (usually indicative of a bacterial or parasitic infection)
- Severe stomach pain, especially when it is concentrated in one area
- Other infections that accompanies the diarrhoea such as pneumonia or ear infections
- History of eating wild mushrooms or any other form of toxins
Do not be anxious about anything, but in every situation, by prayer and petition, with thanksgiving, present your requests to God.
Phil 4:6
The severity of the diarrhoea and vomiting, and associated fluid loss, can vary greatly. Here are some complications to look out for:
Dehydration is the biggest complication associated with diarrhoea, so be sure to look out for the following symptoms:
Mild dehydration starts with the child feeling thirsty or drinking fluids eagerly, a dry mouth and passing slightly less urine. This can still be managed at home.
If your child loses more fluids, they could also have sunken eyes and a sunken fontanelle (soft spot on their head). They can be irritated and pass very little urine. At this stage it is better to see a doctor to make sure you can keep up with the fluid intake.
If the fluid losses continue without replacement, children become sleepy or unresponsive, they pass no urine and they go into a state of shock where there is insufficient blood circulation to the important organs of the body. This is a medical emergency and they need intravenous fluids to catch up with the losses.
Hyponatremia or Hypokalemia (too little salts in the blood) is another possible complication of severe diarrhoea because of the movement of water and salts over the bowel wall. This can cause muscle weakness, cramps, headaches, confusion, convulsions and heart dysrhythmias.
Hypoglycaemia (low blood sugar) could complicate diarrhoea as the little ones often does not want to eat and does not absorb food well while their bowels are ill. This could also cause irritability, convulsions and loss of consciousness.
Intermittent diarrhoea (also called persistent diarrhoea if more than 14days) is mostly due to a combination of factors. When you have a severe bout of infectious diarrhoea the inflammation causes damage to the bowel wall, thus decreasing the absorption of sugars and water. Your child could thus have a type of “lactose intolerance” while the bowel wall is being restored and this causes a prolonged episode of diarrhoea.
When it seems like the diarrhoea will never end, it is probably chronic, and the causes are very different. Do not fear, help is near! I will discuss chronic diarrhoea and the management of fluid loss and diarrhoea in my next blog post!
- Jenkins R, Whyte LA; “Pathophysiology of diarrhoea”; Paediatrics and Child Health Volume 22, Issue 10, October 2012, Pages 443-447
- Elliot EJ; “Acute gastroenteritis in children”; BMJ; 2007 Jan 6; 334(7583):35-40
- http://www.uptodate.com

One thought on “Vomit – Poop – Repeat.”