
When I was 12years old my little brother (2yrs old) woke up from his nap with a fever. It was a very hot and humid afternoon, a thunderstorm was brewing. He was sitting on my mom’s lap, eating a snack when he suddenly started convulsing. He had a febrile seizure that stopped within a few minutes, but those minutes were filled with panic and anxiety and felt like hours!
I know it can be very distressing when your child has a febrile seizure, so I want to equip you with knowledge about febrile seizures, and explain what to do when it happens. I hope I can calm your fears, because it really is not as bad as it looks…

A seizure or convulsion is defined as a febrile seizure if
- child between the ages of 6m – 5years,
- is associated with a fever (>38°C)
AND
- there is no evidence of an infection or other abnormalities of the Central Nervous System
- no metabolic disturbance
- not known with epilepsy
It can be classified as SIMPLE (short duration, generalized tonic-clonic seizure with all limbs involved, single seizure) or COMPLEX (longer than 10min duration, different type of seizure affecting only one arm or leg, multiple seizures in 24hrs).
The peak incidence is in children between 12months and 18months of age. It is mostly associated with viral infections.
Risk factors (who is more likely to get febrile seizures?)
- Genetics: Family history of febrile seizures / other forms of epilepsy
- Inadequate brain growth or weight gain during pregnancy
- Mother smoked / stressed a lot during pregnancy
- Prolonged admission to NICU
- Developmental delay in child
- Viral infections are documented in up to 80% of febrile seizures (Especially Influenza A+B, Adenovirus, Parainfluenza virus, Rhinovirus, Enterovirus, Human Herpes 6 virus)
- Iron or Zinc deficiency
Do not be anxious about anything, but in every situation, by prayer and petition, with thanksgiving, present your requests to God.
Phil 4:6 NIV
Why does it happen?
The exact cause is still unknown, but from what we do understand it looks like a combination of genes, the immature brain of a child, the fever and the fever’s cause all plays a role in triggering a seizure. Genetic mutations or early insults to the brain changes how the brain cells maintain the balance between firing and suppressing the electrical signals between them, and how sensitive the brain cells are to an increase in electrical signals. Increasing the temperature of the brain can also increase neuronal firing which can lead to seizures.
Seizures can also be triggered via the inflammatory pathway. Certain inflammatory markers increase in the blood (usually in response to a viral infection) to tell the body to increase the temperature to assist in the immune-“attack” against an intruder, but these inflammatory markers can also play a role in irritating the brain cells.
Should you worry??
Good News: only 2-5% of children will get febrile seizures. Simple febrile seizures will not cause any damage, most of these children will have normal growth and development with no long term problems!
If a febrile seizure continues for more than 30min it is called a Febrile Status Epilepticus which may be dangerous.
About 40% of children with a first episode of febrile seizures can have a recurrence with a subsequent febrile illness.
Risk factors for recurrence include
- complex febrile seizures,
- family history of febrile seizures,
- less than 18 months of age,
- temperature lower than 40.0°C at first convulsion and
- less than 1 hour between onset of febrile illness and first convulsion
Long term epilepsy develops in 2 to 4% of children with a history of febrile seizures (luckily also very rare).
What should you do when your baby / child has a febrile seizure?

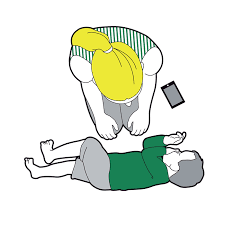



- Breathe – make sure you remain calm so that you can help your child.
- Turn your child into the “recovery position” in a safe space on pillows or the floor. Do not put anything in his / her mouth.
- Watch and Wait for 2mins – most febrile seizures only last for a couple of seconds before terminating spontaneously. Look at which limbs are involved, look at the eyes and the face and if the child is still conscious or not.
- Call for help – if the seizure lasts for longer than 2min go to your local emergency room asap or phone an ambulance.
- See a doctor – even if the seizure was very short and your child is awake, go to see a doctor for further investigations and to confirm the diagnosis.
For simple febrile seizures, no further investigations are necessary to confirm the diagnosis. It is not necessary to do bloods, a CT or an EEG.
In babies 6-18 months old, a lumbar puncture should be done to rule out meningitis if there is any clinical suspicion or if there is no other clue for the cause of the fever.
Other investigations are usually done to determine the cause of the fever or to exclude other problems in Complex febrile seizures.
Management:
The ambulance personnel or ER doctor will give your child a Benzodiazepine (eg Diazepam or Lorazepam) to stop the seizure if they see that your child is still convulsing.
Your child may be admitted for monitoring if he/she is very drowsy after the seizure.
In a future fever episode it is important to manage the fever by giving regular antipyretic medication, however this has not been proven to always prevent future febrile seizures.
Be sure to read my blogpost about fever and how to manage it here.
Have you seen a febrile seizure in a child? Are you comfortable managing your baby with fever at home? What causes you the most distress?
- Francis, J.R., Richmond, P., Robins, C. et al. An observational study of febrile seizures: the importance of viral infection and immunization. BMC Pediatr 16, 202 (2016). https://doi.org/10.1186/s12887-016-0740-5
- Sawires R, Buttery J, Fahey M; “A Review of Febrile Seizures: Recent Advances in Understanding of Febrile Seizure Pathophysiology and Commonly Implicated Viral Triggers”; Front. Pediatr,; 13 Jan 2022; Sec Pediatric Neurology. https://doi.org/10.3389/fped.2021.801321
- Seinfeld DOS, Pellock J; “Recent Research on Febrile Seizures : A Review”; J Neurol Neurophysiol. 2013 Sept 25; 4(165):19519. doi: 10.4172/2155-9562.1000165
